Liver dysfunction may not only reduce the plasma clearance of a number of drugs eliminated by biotransformation and/or biliary excretion, but it can also affect plasma protein binding which in turn could influence the processes of distribution and elimination.
How does liver problem affect drugs in the body?
The capacity of the liver to metabolise drugs depends on hepatic blood flow and liver enzyme activity, both of which can be affected by liver disease. In addition, liver failure can influence the binding of a drug to plasma proteins.
How do diseases of the liver affect metabolism of drugs?
Liver dysfunction not only reduces the clearance of a drug metabolized through hepatic enzymes or biliary mechanisms, but also affects plasma protein binding due to reduced synthesis of albumin and other drug-binding proteins. Even mild-to-moderate hepatic disease may cause an unpredictable effect on drug metabolism.
How does liver cirrhosis affect drug excretion?
In liver cirrhosis the reduced drug elimination is a result of the blood flow through the liver, hepatocytes function and volume of hepatic tissue. Pharmacokinetic and pharmacodynamic changes depend on the nature and degree of hepatic impairment and on the characteristics of the dosed drug.How does the liver eliminate drugs?
Excretion in the bile is another significant form of drug elimination. The liver can actively secrete ionized drugs with a molecular weight greater than 300 g/mol into bile, from where they reach the digestive tract and are either eliminated in feces or reabsorbed as part of the enterohepatic cycle.
How does liver disease affect bioavailability?
Hepatic disease might alter (increase) bioavailability by either or both of 2 mechanisms: decreased hepatic extraction due to impaired hepatic drug metabolising activity, or portosystemic shunting.
How does disease affect drug action?
The absorption, distribution, metabolism, and elimination (ADME) of drugs can be influenced by the physiological and biochemical changes that occur due to various diseases. These changes can have dramatic influence on the exposure of drugs and lead to drug toxicity or lack of drug efficacy.
How can decreased liver and kidney function affect medication action?
Safe medication use, however, is usually most dependent on the condition of patients’ kidneys and livers. Organ dysfunction may decrease drug or drug metabolite excretion in phase 1 or phase 2 drug metabolism reactions (See Table), leading to accumulation and potential toxicity.What is the impact of cirrhosis on drug levels and dosing?
Moreover, patients with cirrhosis are more vulnerable to certain adverse drug reactions (ADRs), such as effects on coagulation or nephrotoxicity. In patients with liver cirrhosis, 20% of the drugs are dosed incorrectly and almost 30% of patients with cirrhosis suffer ADRs.
Does liver disease increase distribution of acidic drugs?Acidic drugs are mainly bound to albumin, whereas basic or neutral drugs are mainly bound to AAG [Israili and Dayton, 2001]. Liver diseases can alter protein binding, tissue binding and fluid levels, thus impacting drug distribution.
Article first time published onHow does kidney disease affect drug elimination?
Since severe renal disease causes a reduction in the plasma protein binding of many drugs, the metabolic clearance of such drugs will be increased.
What principal role does the liver play in drug pharmacokinetics?
Most drugs must pass through the liver, which is the primary site for drug metabolism. Once in the liver, enzymes convert prodrugs to active metabolites or convert active drugs to inactive forms. The liver’s primary mechanism for metabolizing drugs is via a specific group of cytochrome P-450 enzymes.
What altered absorption of some drugs?
Reduced or delayed drug absorption is generally attributed, at least in part, to delayed stomach-emptying due to food. Increased absorption may also result from delayed stomach-emptying facilitating greater drug dissolution before it passes from the stomach into the small intestine.
What factors affect drug absorption metabolism and elimination?
There are four factors that will influence the pharmacokinetic drugs test: water-solubility; fat-soluble; dissociation degree and molecular weight. Pharmacokinetic is a quantitative study of drugs in the body absorption, distribution, metabolism and excretion of the law.
What are 4 factors that affect absorption of a drug?
- physicochemical properties (e.g. solubility)
- drug formulation (e.g. tablets, capsules, solutions)
- the route of administration (e.g. oral, buccal, sublingual, rectal, parenteral, topical, or inhaled)
- the rate of gastric emptying.
What are the factors that influence drug abuse?
- Family history of addiction. Drug addiction is more common in some families and likely involves genetic predisposition. …
- Mental health disorder. …
- Peer pressure. …
- Lack of family involvement. …
- Early use. …
- Taking a highly addictive drug.
What factors affect drug response?
Drug response can be impacted by several factors including diet, comorbidities, age, weight, drug–drug interactions, and genetics. Individual genetic variation in key genes involved in the metabolism, transport, or drug target can contribute to risk of adverse events108 or treatment failure.
How does liver damage affect the first pass effect?
The liver metabolizes many drugs, sometimes to such an extent that only a small amount of active drug emerges from the liver to the rest of the circulatory system. This first pass through the liver thus may greatly reduce the bioavailability of the drug.
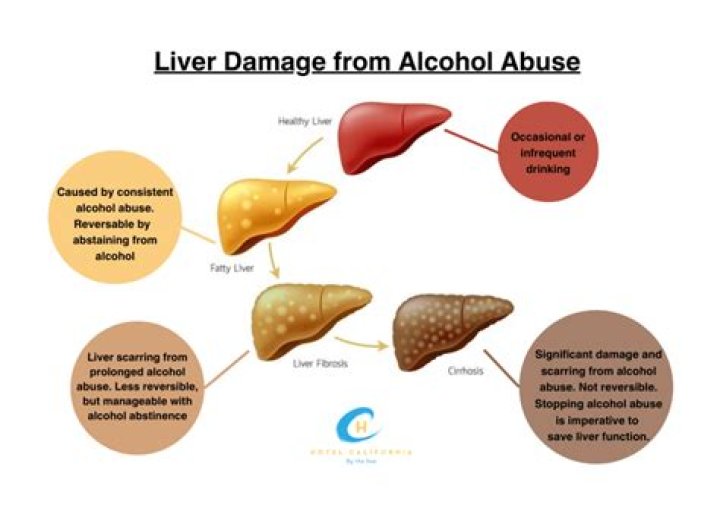
What is the effect of cirrhosis?
Cirrhosis slows the normal flow of blood through the liver, thus increasing pressure in the vein that brings blood to the liver from the intestines and spleen. Swelling in the legs and abdomen. The increased pressure in the portal vein can cause fluid to accumulate in the legs (edema) and in the abdomen (ascites).
What drugs are expected to be used in a patient with liver cirrhosis?
The main treatment for primary biliary cirrhosis is to slow liver damage with the drug ursodiol (Actigall, Urso).
How does liver disease cause encephalopathy?
Hepatic encephalopathy is a nervous system disorder brought on by severe liver disease. When the liver doesn’t work properly, toxins build up in the blood. These toxins can travel to the brain and affect brain function. People with hepatic encephalopathy may seem confused.
How does kidney failure affect the liver?
Hepatorenal syndrome (HRS) is a type of progressive kidney failure seen in people with severe liver damage, most often caused by cirrhosis. As the kidneys stop functioning, toxins begin to build up in the body. Eventually, this leads to liver failure.
Will a drug that is exclusively metabolised by the liver be affected by renal failure?
Renal failure has been shown to alter the hepatic microsomal mixed-function oxidase system of drug metabolizing enzymes. Therefore, in end-stage renal failure, the potential exists for the modification of the disposition of drugs whose elimination is primarily hepatic.
Does CKD affect the liver?
The most important chronic liver diseases associated with chronic renal disease are hepatitis B and C. Several types of renal disease have been recognized: mixed cryoglobulinemia, membranoproliferative glomerulonephritis, membranous nephropathy and polyarteritis nodosa.
Why do drugs excreted unchanged in urine?
Such drugs will therefore be excreted unchanged in the urine because they do not need to undergo biotransformation to increase their water solubility. Active secretion into the renal tubules occurs for some drugs that are not readily filtered in the glomerulus.
What does the liver do?
Functions of the liver All the blood leaving the stomach and intestines passes through the liver. The liver processes this blood and breaks down, balances, and creates the nutrients and also metabolizes drugs into forms that are easier to use for the rest of the body or that are nontoxic.
Do intravenous drugs go through the liver?
Eventually the vasculature redistributes the drug back to the liver through the hepatic artery. First pass metabolism determines what fraction of an oral dose will reach the circulation – the bioavailable fraction. Intravenous drugs don’t experience this first pass effect and are, by definition, 100% bioavailable.
Which pharmacokinetic parameter would hepatic disease most likely affect?
Hepatic impairment is likely to significantly alter the pharmacokinetics (especially metabolism and biliary excretion) of the drug and/or its active metabolites and • A posology adjustment may be needed for such patients taking into account the PK/PD relationship.
What route of drug absorption has the greatest bioavailability?
Intravenous (IV) drug administration is assumed to be the most dependable and accurate route for drug delivery, with a bioavailability of 100%. Absorption of drugs from tissues and organs (e.g., intramuscular, transdermal, rectal) can also be affected by development ( Table 73.2 ).
What factors affect pharmacokinetics of drugs?
Pharmacokinetics can vary from person to person and it is affected by age, gender, diet, environment, body weight and pregnancy, patient’s pathophysiology, genetics and drug- drug or food-drug interactions.
Which enzyme is responsible for the metabolism of drugs in the liver during first pass metabolism?
Although a spectrum of drug biotransformations can occur during first-pass, the most common are oxidations catalyzed by cytochromes P450. It is the isozymes CYP2D6, CYP3A4, CYP1A2, CYP2C9 and CYP2C19 that are most often implicated in first-pass drug elimination.