Pseudohyponatremia is an uncommonly encountered laboratory abnormality defined by a serum sodium concentration of less than 135 mEq/L in the setting of a normal serum osmolality (280 to 300 mOsm/kg).
How is Pseudohyponatremia detected?
Pseudohyponatremia is an artefact; measured serum sodium is reduced but actual plasma sodium is normal. The condition can only arise if the serum lipid or protein concentration is markedly increased and plasma sodium is measured using either indirect ISE or flame photometer.
How is Dilutional hyponatremia diagnosed?
Some of the tests that may be run to help determine which form of hyponatremia a person has include: Blood urea, potassium, calcium, magnesium and phosphate. Plasma and urine osmolality. In dilutional hyponatremia, the plasma osmolality is lower than normal.
How is Euvolemia diagnosed?
- Patients with severely reduced GFR.
- Patients taking thiazides.
- Other patients. – Patients with edema and/or ascites. – Nonedematous patients. Apparent hypovolemia. Apparent euvolemia. – Low urine sodium and osmolality. – High urine sodium and osmolality. – Low urine sodium with high urine osmolality.
How does hyperlipidemia cause hyponatremia?
In states of hyperproteinemia or hyperlipidemia, there is an increased mass of the nonaqueous components of serum and a concomitant decrease in the proportion of serum composed of water. Thus, pseudohyponatremia results because the flame photometry method measures sodium concentration in whole plasma.
How can you tell if someone is hypovolemic?
- Rapid heartbeat.
- Quick, shallow breathing.
- Feeling weak.
- Being tired.
- Confusion or wooziness.
- Having little or no pee.
- Low blood pressure.
- Cool, clammy skin.
How does DKA correct hyponatremia?
In a patient with low or normal serum and DKA, normal saline is the fluid of choice [2]. Normal saline will cause intravascular expansion and correct the hyperosmolar hypovolemic hyponatremia seen in these patients.
How do you investigate hyponatremia?
Overall, serum osmolality and urinary sodium measurements are integral to the diagnosis and management of hyponatremia. Also required are clinical assessment and additional laboratory investigations that may include measuring urine osmolality, serum aldosterone, cortisol, and natriuretic peptide levels.What labs do you order for hyponatremia?
There are three essential laboratory tests in the evaluation of patients with hyponatremia that, together with the history and the physical examination, help to establish the primary underlying etiologic mechanism: urine osmolality, serum osmolality, and urinary sodium concentration.
How can you distinguish between Pseudohyponatremia and hyponatremia?For hyponatremia, serum osmolality is necessary to characterize the low sodium level further. Pseudohyponatremia is associated with normal serum osmolality, which is defined as a value between 280 and 300 mOsm/kg.
Article first time published onHow do you read hyponatremia labs?
A urine osmolality value of less than 100 mOsm/kg indicates complete and appropriate suppression of antidiuretic hormone secretion. A urine sodium level less than 20 mmol/L is indicative of hypovolemia, whereas a level greater than 40 mmol/L is suggestive of the syndrome of inappropriate antidiuretic hormone secretion.
How do you assess volume status in hyponatremia?
Although volume status is difficult to assess with any accuracy at the bedside, a clinical assessment with attention to the patient’s history, heart rate, blood pressure, jugular venous pressure, the presence of pedal and sacral edema, the presence of a postural drop, and point-of-care ultrasound is usually adequate to …
How do you test for Hypernatremia?
Hypernatremia is often diagnosed through blood tests. Urine tests can also be used to identify high levels of sodium along with urine concentration. Both blood and urine tests are fast, minimally invasive tests that require no preparation. Hypernatremia tends to develop as a result of underlying conditions.
How do pediatrics correct hyponatremia?
In patients with normovolemic hyponatremia, restriction of fluids to two-thirds (or less) of the volume needed for maintenance is the mainstay of treatment. Diuretics can be administered with fluid restriction to remove excessive free water. Once again, the change in Na levels should not exceed 8 mEq/L/d.
How do I test my sodium levels?
A blood test can help your doctor check for low sodium levels. Even if you don’t have symptoms of low blood sodium, your doctor may order a basic metabolic panel. This tests the amounts of electrolytes and minerals in your blood. A basic metabolic panel is often part of a routine physical.
How does glucose cause Pseudohyponatremia?
Hyperglycemia causes osmotic shifts of water from the intracellular to the extracellular space, causing a relative dilutional hyponatremia.
Do you code Pseudohyponatremia?
As such, pseudohyponatremia cannot be coded, and coding efforts should focus on identifying the inciting cause.
Does hyperlipidemia cause low potassium?
Hyperlipidemia is prevalent in hypertension, but the cause of this association is unknown. Treatment of hypertension with thiazide diuretics accentuates the hyperlipidemia, perhaps by causing potassium or sodium depletion.
What happens to serum sodium in DKA?
High serum osmolarity also drives water from intracellular to extracellular space, causing dilutional hyponatremia. Sodium also is lost in the urine during the osmotic diuresis.
Is sodium high or low in DKA?
The osmotic diuresis is associated with large losses of electrolytes in the urine. The sodium chloride deficit in DKA and HHS is usually 5–13 mmol/kg of body weight for sodium and 3–7 mmol/kg for chloride1,4,7 (Table 1).
How is hyperosmolar hyperglycemic state diagnosed?
- Plasma glucose level of 600 mg/dL or greater.
- Effective serum osmolality of 320 mOsm/kg or greater.
- Profound dehydration, up to an average of 9 L.
- Serum pH greater than 7.30.
- Bicarbonate concentration greater than 15 mEq/L.
How do you assess for Hypervolemia?
The key diagnostic signs of hypervolemia include weight gain and swelling. One or more parts of your body may appear swollen, depending on whether or not you have been sitting, lying, or standing before your visit. Your doctor is also likely to perform a blood test to check your sodium levels.
What labs indicate hypovolemia?
blood urea/plasma creatinine ratio is 1:10 or less (For example, a ratio of 1:5 would suggest hypovolemia) Page 2 b.
What clinical manifestations would indicate maternal hypovolemic shock?
Decreased or no urine output. Generalized weakness. Pale skin color (pallor) Rapid breathing.
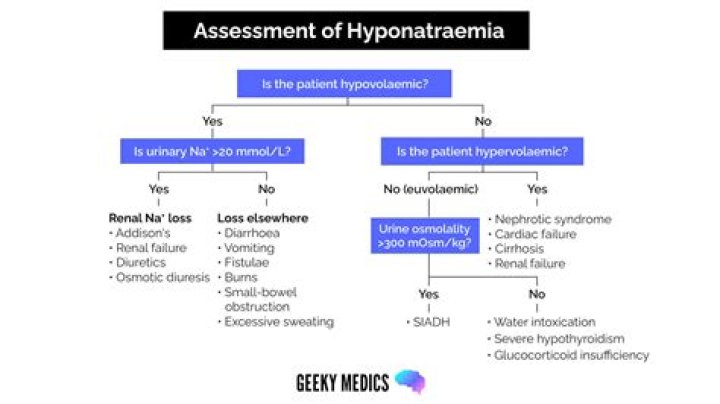
Which clinical features should be assessed in all patients with hyponatraemia to help determine the underlying cause?
Experts agree that measurement of serum osmolality, urine osmolality, and urine sodium concentration help to determine the underlying cause of hyponatraemia [Ball, 2016; BMJ, 2019], particularly in the absence of clear comorbidities [Saeed, 2014].
What drugs cause hyponatraemia?
- Angiotensin-converting enzyme inhibitors (ACE inhibitors)
- Heparin.
- Diuretics.
- Antidepressants.
- Antipsychotics.
- Carbamazepine.
- Eslicarbazepine.
- Oxcarbazepine.
When do you admit low sodium?
When is hyponatraemia a medical emergency? Hyponatraemia of rapid onset (fall of <10mmol/L within 48h) and/or symptoms of cerebral oedema should be treated as a medical emergency – the patient should be admitted to hospital.
How is serum osmolality measured?
Serum osmolality is measured using a technique called osmometry. The most widely used method of osmometry is freezing-point depression, for which a value is obtained based on the temperature at which the serum sample freezes. Another method used to measure serum osmolality is vapor pressure osmometry.
What is normal serum osmolality?
Normal Results Normal values range from 275 to 295 mOsm/kg (275 to 295 mmol/kg). Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or test different samples.
What is Hypoosmolar hyponatremia?
Hypoosmolar hyponatremia is a condition where hyponatremia associated with a low plasma osmolality. The term “hypotonic hyponatremia” is also sometimes used. When the plasma osmolarity is low, the extracellular fluid volume status may be in one of three states: low volume, normal volume, or high volume.
What is normal level of sodium in urine?
For adults, normal urine sodium values are generally 20 mEq/L in a random urine sample and 40 to 220 mEq per day.