Focus Charting – is a method for organizing health information in the individual’s record. It is a systematic approach to documentation, using nursing terminology to describe individual’s health status and nursing action. Focus.
What is the primary purpose of focus charting?
Focus charting describes the patient’s perspective and focuses on documenting the patient’s current status, progress towards goals and response to interventions. Focus charting brings the focus of care back to the patient and the patients’ concerns.
What does focus stand for in nursing?
FOCUS is an acronym for the words find, organise, clarify, understand, and select. PDCA is an acronym for plan, do, act, and check results.
What is focused reporting charting?
Definition. Focus Charting of F-DAR is intended to make the client and client concerns and strengths the focus of care. It is a method of organizing health information in an individual’s record. Focus Charting is a systematic approach to documentation.What is DAR format?
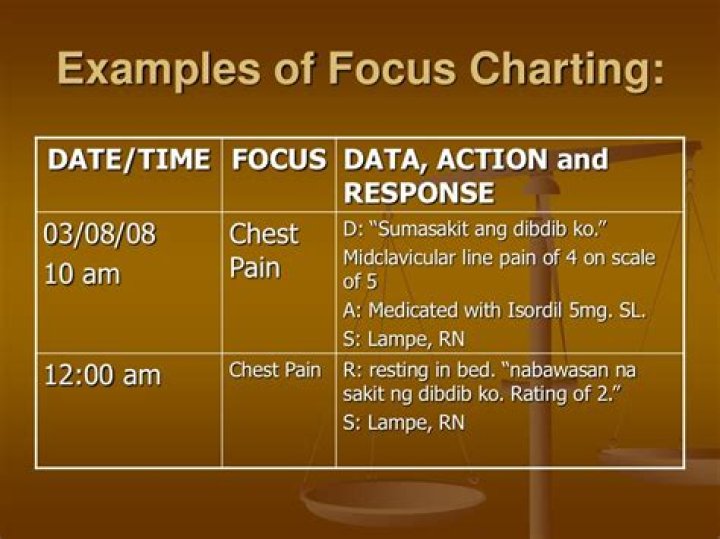
DAR is an acronym that stands for data, action, and response. Focus charting assists nurses in documenting patient records by providing a systematic template for each patient and their specific concerns and strengths to be the focus of care. DAR notes are often referred to without the F.
How do nurses chart?
- Do memorize your workplace’s policies. …
- Don’t be “too busy” for accurate charting. …
- Do write legibly and learn abbreviations. …
- Don’t include your opinion. …
- Do ask questions. …
- Don’t chart in advance.
What does chart by exception mean?
Charting by Exception Framework When a healthcare provider charts by exception, it means that only exceptions to these baseline findings would be charted. If nothing was charted, the patient’s status is assumed to match the baseline. … Providers who find this in the patient’s exam would not need to chart this.
What is narrative charting?
Narrative charting, the traditional form of nursing documentation, is a story format documenting client status, interventions, treatments, and responses. … Source-oriented (SO) charting is a narrative recording by each member (source) of the health care team charts on separate records.What is soap charting in nursing?
Nurses and other healthcare providers use the SOAP note as a documentation method to write out notes in the patient’s chart. SOAP stands for subjective, objective, assessment, and plan.
Why is FDAR important?What is F-DAR charting and why it is used? It is a method of charting nurses use, along with other disciplines, to help focus on a specific patient problem, concern, or event. It is geared to save time and decrease duplicate charting.
Article first time published onWhat are the methods for documenting nurses notes in the Philippines?
There are many different methods of documentation including but not limited to: narrative charting, source-oriented charting, problem-oriented charting (SOAP/SOAPIE), • problem-intervention-evaluation charting (PIE), • focus charting (DARP-Data, action, response, plan), • critical pathways, and • charting by exception.
What does focus mean in medical terms?
foci (fō’kŭs, -sī) 1. The point at which the light rays meet after passing through a convex lens. 2. The center, or the starting point, of a disease process.
What are the focus in medical field?
Medicine is the field of health and healing. It includes nurses, doctors, and various specialists. It covers diagnosis, treatment, and prevention of disease, medical research, and many other aspects of health. Medicine aims to promote and maintain health and wellbeing.
What is the full form of focus?
Abbreviation : FOCUS FOCUS – Future Opportunities Careers And Ultimate Success.
What are some common charting formats?
A variety of forms are used in the patient record, including admission data forms, discharge summary, flow sheets, graphic records, checklists, medication administration records, intake and output records, care plans, and Kardex.
What are the do's and dont's of documentation?
DON’T copy information. Write each transport as if this is the first time you have seen or treated this patient. Do not copy information, especially your narrative, from a previous report.
What is a pie Note nursing?
PIE Acronym for a process-oriented documentation system. The progress notes in the patient record use (P) to define the particular P roblem; (I) to document I ntervention; and (E) to E valuate the patient outcome. PIE charting integrates care planning with progress notes.
Why do nurses chart by exception?
CHARTING BY EXCEPTION (CBE) or variance charting is a system for documenting exceptions to normal illness or disease progression, using a shorthand method of charting what’s usual and normal. … You need to make additional documentation when the patient’s condition deviates from the standard or what’s expected.
What is defensive charting?
Defensive Documentation: Steps Nurses Can Take to Improve Their Charting and Reduce Their Liability. … Documentation provides a picture of the patient’s condition and how they respond to treatment, which influences the decisions that subsequent providers will make regarding the patient’s care.
Is charting by exception acceptable?
Charting by exception: the legal risks. Charting by exception does not necessarily result in patient records that give an incomplete picture, but minimizing documentation is risky. … A lack of detail could compromise patient safety as well.
How do you write a nursing progress note?
- Date and time of the report.
- Patient’s name.
- Doctor and nurse’s name.
- General description of the patient.
- Reason for the visit.
- Vital signs and initial health assessment.
- Results of any tests or bloodwork.
- Diagnosis and care plan.
What is chart in nursing notes?
Nurse charting should include context, though. Shafer says to “include details about patient teaching, family interaction and anything that you would want to know about the interaction and care you provided if you were to encounter the chart five years from now.”
How do you document patient fall?
- how the patient was discovered and all known facts regarding the fall.
- assessment of the patient.
- notification of the patient’s physician. any orders that were given have been carried out and patient’s response to them.
How can I improve my charting?
- Know what are you trying to show. Before you get to chart-making be sure you know what your goal is. …
- Use charts like sentences. …
- Charts should make sense in isolation. …
- Don’t make someone work to understand your chart. …
- Remember that not everything should be charted.
Why do nurses chart in third person?
Charting in third-person is considered more formal and professional, and in the case of documenting patient care – this point-of-view reads more objectively (as this type of documentation should be) and puts the patient as the focus of the documentation.
How do you teach SOAP notes?
- Find the appropriate time to write SOAP notes.
- Maintain a professional voice.
- Avoid overly wordy phrasing.
- Avoid biased overly positive or negative phrasing.
- Be specific and concise.
- Avoid overly subjective statement without evidence.
- Avoid pronoun confusion.
- Be accurate but nonjudgmental.
What does the O in soap stand for?
The acronym SOAP stands for Subjective, Objective, Assessment, and Plan.
What is traditional charting?
Narrative Charting – This is the traditional form of charting. It is a source-oriented record wherein each medical personnel makes documentation on the patient’s record in a separate section. The advantage of using this type of recording is the provision of an organized sections for each member of the healthcare team.
What are the methods of charting?
The charting method is a note-taking method that uses charts to condense and organize notes. It involves splitting a document into several columns and rows which are then filled with summaries of information. This results in a note format that enables efficient comparisons between different topics and ideas.
What is traditional charting in nursing?
This is the most familiar method of documenting nursing care. ааIt is a diary or story format in chronological order. It is used to document the patient’s status, care, events, treatments, interventions, and patient’s response to the interventions.
What is data action response?
DAR is a form of focus charting and the dar stands for data-action-response. It ensures documentation that is based upon the nursing process. Routine nursing tasks and assessment data is documented on flow sheets and checklists.